Jun 22, 2026
Mia Bolton
EMR System Connectivity and Integration
EMR System interoperability is one of the highest technical hurdles to a fast and reliable healthcare system. Here, we cover why and how it may be resolved.
Payers today have more access to EMR systems and EMR data than ever before. The focus over the last decade and, still today, is on interoperability for acquisition, not for actionable intelligence or value delivery. Clinical data available in these EMR systems have to answer multiple questions for use cases like risk adjustment, prior authorization, HEDIS, and utilization management, but the challenge is that the data varies dramatically depending on how it's connected and what's done with it.
EMR System Data Authorization
HIPAA, for example, states that healthcare data can only be shared for uses of treatment, payment, and healthcare operations. It states that covered entities can use data for multiple purposes if those purposes are permitted by law.
However, there are limits:
Purpose restrictions - if data has contractual limitations regarding how it was received, it must adhere to those.
Patient authorizations - If data was received under a patient authorization for one purpose, additional purposes may require a new authorization.
Research - Data obtained for a research study may be limited by the study protocol, IRB approval, informed consent language, and the Common Rule.
Minimum necessary - Even when multiple uses are allowed, organizations should access the data for the minimum amount necessary.
State laws - Some states impose stricter purpose limitations than HIPAA.
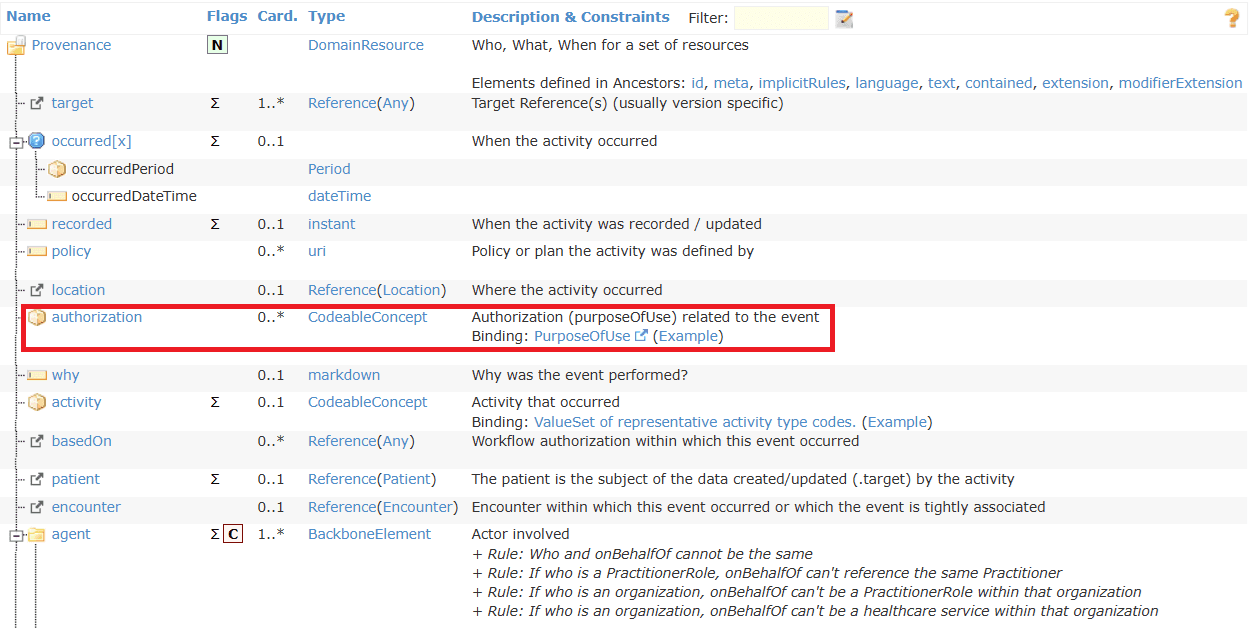
FHIR data supports resources such as Provenance, Consent, and Security Labels that can help organizations track data origin and usage constraints.
EMR System Interoperability Today
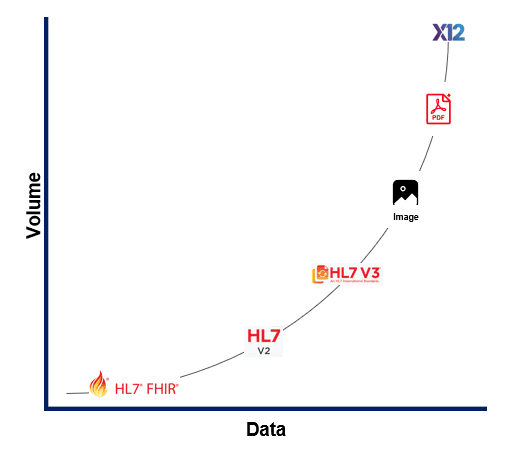
EMR systems today must generate large amounts of documentation and custom mappings used by systems connecting to them. When not using custom field mappings, they permit objects such as CCDA, FHIR, and PDF as payloads and various integration options, like standard-based APIs (ADT/HL7 FHIR v2 messaging), integrations directly to databases, or legacy interfaces to transfer the data and connect systems. ADT/HL7 FHIR v2 is still one of the most prevalent data exchange formats used today between EMR systems, even though the standard has been around for decades and is very narrow in the insights it provides. In more recent years, with the introduction of the CMS Interoperability rules and FHIR R4 APIs, additional standardization on access and connectivity has allowed for some improvement in connectivity and data exchange between EMR systems, but the implementation of these APIs is executed differently across the EMR systems. This creates a fragmented dataset that payers still need to transform or normalize as part of the processing of any data format received through their interoperability connections today.
Healthcare Data Continuum: Complexity and Fragmentation
In addition to the fragmented data received by the EMR systems, data transformation partners have disrupted the current interoperability IT infrastructure built by payers, as these partners usually only tackle one data format at a time. So, not only are payers managing the various connections to EMR systems and other interoperability data channels, they now have to piecemeal data transformation processing across all their connections. This creates a data strategy that is more like a "data dump" of clinical data, versus one that delivers value. To develop a data pipeline that considers and transforms all data formats available in the healthcare system and to manage the quality of their clinical data, payers should consider an AI-powered platform that consolidates EMR system connectivity and transforms raw data into actionable clinical intelligence.
How does “Data Dump" EMR connectivity disrupt value delivery?
As data flows and is requested through the fragmented connectivity infrastructure across EMR systems, the clinical data delivers insight for one or at most two use cases. This inefficiency creates a huge volume of clinical data that sits underutilized in data marts. In addition, the EMR systems' output also presents additional challenges, such as:
Duplication: can be identical medical records, can be identical clinical data from the same encounter, can be identical clinical data across multiple encounters, etc.
Validation: invalid LOINC/SNOWMED codes, placeholder values (strings of 9s or 0s), missing provenance, etc.
Inconsistency: Format across EMR systems vary from PDFs, to images, to nested files, to FHIR
The current ‘data dump’ process Tenasol sees across our customers has created a system built on volume, not value, as health plans are beginning to need not just more connectivity. Payers are looking for a transformation process that encompasses all the dynamics that legacy interoperability has created and a system that can not only integrate across all EHR systems but also transform to a usable standard that will continue to add value.
What does intelligent EMR System connectivity mean for payers?
Now, as payers are beginning to not just build connection points to support their interoperability strategy, but an intelligence layer that can ingest any data format, normalize and transform, deduplicate, and present usable value. This elevates a legacy system from being the data dump of one-use data to an intelligent system that enables clinical data to be multiple-purpose. In building an intelligent EMR connectivity, the following are key in your strategy:
A single integration layer that spans EMR systems (Epic, Cerner, athenahealth, etc.) rather than siloed vendor connections
AI tools that pull discrete clinical findings (diagnoses, medications, procedures, HCC-relevant conditions) from both structured and unstructured EMR data
Deduplication and normalization functionality to remove the noise from the same or different EMR systems
Provenance and auditability, knowing which EMR system, encounter, and practitioner a finding originates from, with traceability to support internal and external audits
How does AI-powered EMR system connectivity deliver value?
The Tenasol Platform creates a singular data pipeline and the one-stop-shop to enable AI-powered connectivity, where plans can develop an intelligent data management system to support enterprise-wide data value.
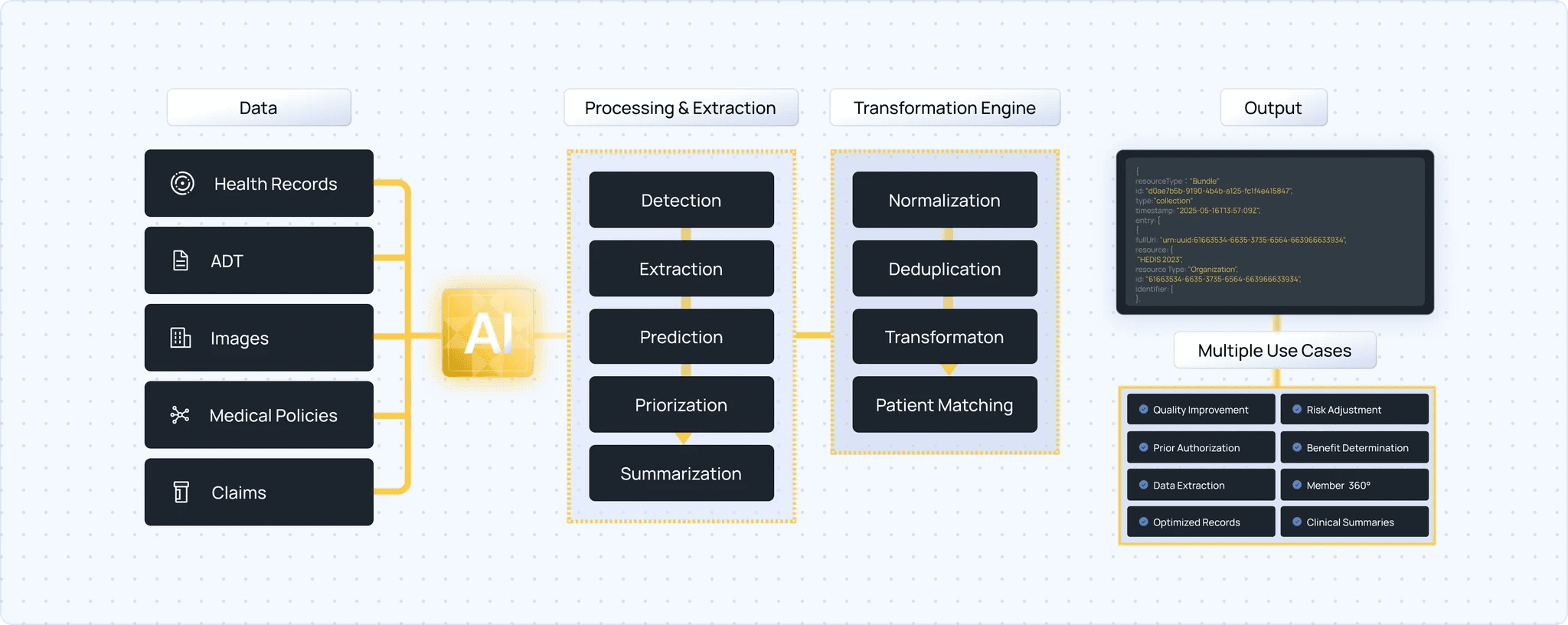
A few examples in how value delivery is seen are:
Risk Adjustment: EMR systems provide longitudinal diagnosis history needed to close HCC gaps. To support gap closure, NLP is the AI-tool that can extract structured findings from unstructured notes.
Prior Authorization: When a prior authorization (PA) request is sent, payers need to access EMR systems in near-real-time. Through consolidated connectivity, one API request delivers an intelligent response if the clinical information across the EMR systems support the PA request or if just the clinical document exists.
HEDIS / Quality Measurement: Many HEDIS numerator and denominator data depend on clinical evidence in EMR systems across one or many encounters per member.
Fragmented EMR data leads to missed measure compliance and inaccurate Star Ratings, as it can be difficult to validate or audit clinical findings against what is present in the original source.
In this new age of intelligent connectivity, the goal has shifted from not just connectivity to EMR systems that deliver data dumps, but consolidating your clinical data processing through an AI-powered data pipeline. This evolution allows for greater clinical clarity that delivers value across the health plan’s enterprise data strategy, leading to reduced costs of care, improved quality outcomes, and enabling more intelligent and faster decisions.
Reach out to our team to learn how Tenasol's AI-powered platform consolidates EMR system connectivity and transforms raw data into actionable clinical intelligence.
EMR System interoperability is one of the highest technical hurdles to a fast and reliable healthcare system. Here, we cover why and how it may be resolved.
Payers today have more access to EMR systems and EMR data than ever before. The focus over the last decade and, still today, is on interoperability for acquisition, not for actionable intelligence or value delivery. Clinical data available in these EMR systems have to answer multiple questions for use cases like risk adjustment, prior authorization, HEDIS, and utilization management, but the challenge is that the data varies dramatically depending on how it's connected and what's done with it.
EMR System Data Authorization
HIPAA, for example, states that healthcare data can only be shared for uses of treatment, payment, and healthcare operations. It states that covered entities can use data for multiple purposes if those purposes are permitted by law.
However, there are limits:
Purpose restrictions - if data has contractual limitations regarding how it was received, it must adhere to those.
Patient authorizations - If data was received under a patient authorization for one purpose, additional purposes may require a new authorization.
Research - Data obtained for a research study may be limited by the study protocol, IRB approval, informed consent language, and the Common Rule.
Minimum necessary - Even when multiple uses are allowed, organizations should access the data for the minimum amount necessary.
State laws - Some states impose stricter purpose limitations than HIPAA.
FHIR data supports resources such as Provenance, Consent, and Security Labels that can help organizations track data origin and usage constraints.
EMR System Interoperability Today
EMR systems today must generate large amounts of documentation and custom mappings used by systems connecting to them. When not using custom field mappings, they permit objects such as CCDA, FHIR, and PDF as payloads and various integration options, like standard-based APIs (ADT/HL7 FHIR v2 messaging), integrations directly to databases, or legacy interfaces to transfer the data and connect systems. ADT/HL7 FHIR v2 is still one of the most prevalent data exchange formats used today between EMR systems, even though the standard has been around for decades and is very narrow in the insights it provides. In more recent years, with the introduction of the CMS Interoperability rules and FHIR R4 APIs, additional standardization on access and connectivity has allowed for some improvement in connectivity and data exchange between EMR systems, but the implementation of these APIs is executed differently across the EMR systems. This creates a fragmented dataset that payers still need to transform or normalize as part of the processing of any data format received through their interoperability connections today.
Healthcare Data Continuum: Complexity and Fragmentation
In addition to the fragmented data received by the EMR systems, data transformation partners have disrupted the current interoperability IT infrastructure built by payers, as these partners usually only tackle one data format at a time. So, not only are payers managing the various connections to EMR systems and other interoperability data channels, they now have to piecemeal data transformation processing across all their connections. This creates a data strategy that is more like a "data dump" of clinical data, versus one that delivers value. To develop a data pipeline that considers and transforms all data formats available in the healthcare system and to manage the quality of their clinical data, payers should consider an AI-powered platform that consolidates EMR system connectivity and transforms raw data into actionable clinical intelligence.
How does “Data Dump" EMR connectivity disrupt value delivery?
As data flows and is requested through the fragmented connectivity infrastructure across EMR systems, the clinical data delivers insight for one or at most two use cases. This inefficiency creates a huge volume of clinical data that sits underutilized in data marts. In addition, the EMR systems' output also presents additional challenges, such as:
Duplication: can be identical medical records, can be identical clinical data from the same encounter, can be identical clinical data across multiple encounters, etc.
Validation: invalid LOINC/SNOWMED codes, placeholder values (strings of 9s or 0s), missing provenance, etc.
Inconsistency: Format across EMR systems vary from PDFs, to images, to nested files, to FHIR
The current ‘data dump’ process Tenasol sees across our customers has created a system built on volume, not value, as health plans are beginning to need not just more connectivity. Payers are looking for a transformation process that encompasses all the dynamics that legacy interoperability has created and a system that can not only integrate across all EHR systems but also transform to a usable standard that will continue to add value.
What does intelligent EMR System connectivity mean for payers?
Now, as payers are beginning to not just build connection points to support their interoperability strategy, but an intelligence layer that can ingest any data format, normalize and transform, deduplicate, and present usable value. This elevates a legacy system from being the data dump of one-use data to an intelligent system that enables clinical data to be multiple-purpose. In building an intelligent EMR connectivity, the following are key in your strategy:
A single integration layer that spans EMR systems (Epic, Cerner, athenahealth, etc.) rather than siloed vendor connections
AI tools that pull discrete clinical findings (diagnoses, medications, procedures, HCC-relevant conditions) from both structured and unstructured EMR data
Deduplication and normalization functionality to remove the noise from the same or different EMR systems
Provenance and auditability, knowing which EMR system, encounter, and practitioner a finding originates from, with traceability to support internal and external audits
How does AI-powered EMR system connectivity deliver value?
The Tenasol Platform creates a singular data pipeline and the one-stop-shop to enable AI-powered connectivity, where plans can develop an intelligent data management system to support enterprise-wide data value.
A few examples in how value delivery is seen are:
Risk Adjustment: EMR systems provide longitudinal diagnosis history needed to close HCC gaps. To support gap closure, NLP is the AI-tool that can extract structured findings from unstructured notes.
Prior Authorization: When a prior authorization (PA) request is sent, payers need to access EMR systems in near-real-time. Through consolidated connectivity, one API request delivers an intelligent response if the clinical information across the EMR systems support the PA request or if just the clinical document exists.
HEDIS / Quality Measurement: Many HEDIS numerator and denominator data depend on clinical evidence in EMR systems across one or many encounters per member.
Fragmented EMR data leads to missed measure compliance and inaccurate Star Ratings, as it can be difficult to validate or audit clinical findings against what is present in the original source.
In this new age of intelligent connectivity, the goal has shifted from not just connectivity to EMR systems that deliver data dumps, but consolidating your clinical data processing through an AI-powered data pipeline. This evolution allows for greater clinical clarity that delivers value across the health plan’s enterprise data strategy, leading to reduced costs of care, improved quality outcomes, and enabling more intelligent and faster decisions.
Reach out to our team to learn how Tenasol's AI-powered platform consolidates EMR system connectivity and transforms raw data into actionable clinical intelligence.
EMR System interoperability is one of the highest technical hurdles to a fast and reliable healthcare system. Here, we cover why and how it may be resolved.
Payers today have more access to EMR systems and EMR data than ever before. The focus over the last decade and, still today, is on interoperability for acquisition, not for actionable intelligence or value delivery. Clinical data available in these EMR systems have to answer multiple questions for use cases like risk adjustment, prior authorization, HEDIS, and utilization management, but the challenge is that the data varies dramatically depending on how it's connected and what's done with it.
EMR System Data Authorization
HIPAA, for example, states that healthcare data can only be shared for uses of treatment, payment, and healthcare operations. It states that covered entities can use data for multiple purposes if those purposes are permitted by law.
However, there are limits:
Purpose restrictions - if data has contractual limitations regarding how it was received, it must adhere to those.
Patient authorizations - If data was received under a patient authorization for one purpose, additional purposes may require a new authorization.
Research - Data obtained for a research study may be limited by the study protocol, IRB approval, informed consent language, and the Common Rule.
Minimum necessary - Even when multiple uses are allowed, organizations should access the data for the minimum amount necessary.
State laws - Some states impose stricter purpose limitations than HIPAA.
FHIR data supports resources such as Provenance, Consent, and Security Labels that can help organizations track data origin and usage constraints.
EMR System Interoperability Today
EMR systems today must generate large amounts of documentation and custom mappings used by systems connecting to them. When not using custom field mappings, they permit objects such as CCDA, FHIR, and PDF as payloads and various integration options, like standard-based APIs (ADT/HL7 FHIR v2 messaging), integrations directly to databases, or legacy interfaces to transfer the data and connect systems. ADT/HL7 FHIR v2 is still one of the most prevalent data exchange formats used today between EMR systems, even though the standard has been around for decades and is very narrow in the insights it provides. In more recent years, with the introduction of the CMS Interoperability rules and FHIR R4 APIs, additional standardization on access and connectivity has allowed for some improvement in connectivity and data exchange between EMR systems, but the implementation of these APIs is executed differently across the EMR systems. This creates a fragmented dataset that payers still need to transform or normalize as part of the processing of any data format received through their interoperability connections today.
Healthcare Data Continuum: Complexity and Fragmentation
In addition to the fragmented data received by the EMR systems, data transformation partners have disrupted the current interoperability IT infrastructure built by payers, as these partners usually only tackle one data format at a time. So, not only are payers managing the various connections to EMR systems and other interoperability data channels, they now have to piecemeal data transformation processing across all their connections. This creates a data strategy that is more like a "data dump" of clinical data, versus one that delivers value. To develop a data pipeline that considers and transforms all data formats available in the healthcare system and to manage the quality of their clinical data, payers should consider an AI-powered platform that consolidates EMR system connectivity and transforms raw data into actionable clinical intelligence.
How does “Data Dump" EMR connectivity disrupt value delivery?
As data flows and is requested through the fragmented connectivity infrastructure across EMR systems, the clinical data delivers insight for one or at most two use cases. This inefficiency creates a huge volume of clinical data that sits underutilized in data marts. In addition, the EMR systems' output also presents additional challenges, such as:
Duplication: can be identical medical records, can be identical clinical data from the same encounter, can be identical clinical data across multiple encounters, etc.
Validation: invalid LOINC/SNOWMED codes, placeholder values (strings of 9s or 0s), missing provenance, etc.
Inconsistency: Format across EMR systems vary from PDFs, to images, to nested files, to FHIR
The current ‘data dump’ process Tenasol sees across our customers has created a system built on volume, not value, as health plans are beginning to need not just more connectivity. Payers are looking for a transformation process that encompasses all the dynamics that legacy interoperability has created and a system that can not only integrate across all EHR systems but also transform to a usable standard that will continue to add value.
What does intelligent EMR System connectivity mean for payers?
Now, as payers are beginning to not just build connection points to support their interoperability strategy, but an intelligence layer that can ingest any data format, normalize and transform, deduplicate, and present usable value. This elevates a legacy system from being the data dump of one-use data to an intelligent system that enables clinical data to be multiple-purpose. In building an intelligent EMR connectivity, the following are key in your strategy:
A single integration layer that spans EMR systems (Epic, Cerner, athenahealth, etc.) rather than siloed vendor connections
AI tools that pull discrete clinical findings (diagnoses, medications, procedures, HCC-relevant conditions) from both structured and unstructured EMR data
Deduplication and normalization functionality to remove the noise from the same or different EMR systems
Provenance and auditability, knowing which EMR system, encounter, and practitioner a finding originates from, with traceability to support internal and external audits
How does AI-powered EMR system connectivity deliver value?
The Tenasol Platform creates a singular data pipeline and the one-stop-shop to enable AI-powered connectivity, where plans can develop an intelligent data management system to support enterprise-wide data value.
A few examples in how value delivery is seen are:
Risk Adjustment: EMR systems provide longitudinal diagnosis history needed to close HCC gaps. To support gap closure, NLP is the AI-tool that can extract structured findings from unstructured notes.
Prior Authorization: When a prior authorization (PA) request is sent, payers need to access EMR systems in near-real-time. Through consolidated connectivity, one API request delivers an intelligent response if the clinical information across the EMR systems support the PA request or if just the clinical document exists.
HEDIS / Quality Measurement: Many HEDIS numerator and denominator data depend on clinical evidence in EMR systems across one or many encounters per member.
Fragmented EMR data leads to missed measure compliance and inaccurate Star Ratings, as it can be difficult to validate or audit clinical findings against what is present in the original source.
In this new age of intelligent connectivity, the goal has shifted from not just connectivity to EMR systems that deliver data dumps, but consolidating your clinical data processing through an AI-powered data pipeline. This evolution allows for greater clinical clarity that delivers value across the health plan’s enterprise data strategy, leading to reduced costs of care, improved quality outcomes, and enabling more intelligent and faster decisions.
Reach out to our team to learn how Tenasol's AI-powered platform consolidates EMR system connectivity and transforms raw data into actionable clinical intelligence.




GET STARTED NOW
Leverage the Power of AI with Tenasol Today!

Powered by AI,
Purpose Built for Healthcare

Contact Information
2461 Eisenhower Avenue, 2nd Floor
Alexandria, VA 22314
Phone: (202) 888-1757
© 2026 Tenasol. All rights reserved.



Disclaimer:
The information and materials on this website are provided for general informational purposes only and are subject to change without notice. We make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability, or availability of the website or its content. Any reliance you place on such information is strictly at your own risk. We are not responsible for, and do not necessarily endorse, the content of any third-party websites linked from this site. All product names, logos, and brands are property of their respective owners.
Powered by AI,
Purpose Built for Healthcare
Contact Information
2461 Eisenhower Avenue, 2nd Floor
Alexandria, VA 22314
Phone: (202) 888-1757
© 2026 Tenasol. All rights reserved.
Disclaimer:
The information and materials on this website are provided for general informational purposes only and are subject to change without notice. We make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability, or availability of the website or its content. Any reliance you place on such information is strictly at your own risk. We are not responsible for, and do not necessarily endorse, the content of any third-party websites linked from this site. All product names, logos, and brands are property of their respective owners.
Powered by AI,
Purpose Built for Healthcare
Contact Information
2461 Eisenhower Avenue, 2nd Floor
Alexandria, VA 22314
Phone: (202) 888-1757
© 2026 Tenasol. All rights reserved.
Disclaimer:
The information and materials on this website are provided for general informational purposes only and are subject to change without notice. We make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, suitability, or availability of the website or its content. Any reliance you place on such information is strictly at your own risk. We are not responsible for, and do not necessarily endorse, the content of any third-party websites linked from this site. All product names, logos, and brands are property of their respective owners.